
The Enhanced Oncology Care Model and What it Means for Participating Oncology Practices
On Monday June 27, 2022, the Center for Medicare and Medicaid Innovation (CMMI) released a Request for Applications (RFA) for the Enhancing Oncology Model (EOM), the successor alternative payment model (APM) to the Oncology Care Model (OCM), which concluded with episodes ending by June 30, 2022.
Oncology practices have been waiting for CMMI to unveil their new oncology value-based care model. And while the EOM is, in many respects, structurally similar to its predecessor, as Dr. Stephen Schleicher, MD, MBA, Chief Medical Officer for Tennessee Oncology, briefly described in an OBR editorial commentary on June 28, 2022 the new model has notable differences from its predecessor.
In this post, we offer an analysis of the differences between the two models and the anticipated impact on the physician practice groups (PGPs) that elect to participate. And in a subsequent post, we will highlight some of the key strategic considerations that practices should consider in the decision of whether to participate.
Submitting the Application Preserves Practices’ Future Options
It’s worth noting that EOM is scheduled to launch on July 1, 2023 and is intended to be a 5-year voluntary payment model. To retain the option to participate in EOM, oncology PGPs must submit to complete the application process by September 30, 2022.
Submitting an application does not bind an applicant to participate in EOM, but it will allow PGPs that apply to uncover further details regarding the EOM and how they might eventually perform in the model. For example, accepted applicants will have to sign a full Participation Agreement with CMS, which will likely be issued to accepted applicants in late 2022 or early 2023. In addition, accepted applicants will be eligible to receive baseline period claims data files that will provide insight their historical cost trends.
These are just a couple of examples of information that will be critical for PGPs to consider in their decision to participate in EOM that requires the submission of an application by the September 30th deadline.
Included Medicare Patient Population
A fundamental difference between the OCM and EOM is the Medicare population included in the model. While OCM included Medicare beneficiaries that received any form of systemic anticancer therapy for any of 21 cancer types; EOM will only include beneficiaries with any of seven of the more prevalent cancer types (breast cancer, lung cancer, lymphoma, multiple myeloma, small intestine/colorectal, prostate cancer, and chronic leukemia). It’s also worth noting that breast cancer (patients receiving only hormonal therapy (i.e. those defined as “low-risk” breast cancer in OCM) would not be included in EOM.
Impact
Limiting the diagnoses included in EOM will significantly decrease the population of patients in the model relative to OCM with commensurately significant decreases in Monthly Enhanced Oncology Services (MEOS) payments that EOM participants would be eligible to receive under the program. This means that the investments and efforts that participants make in implementing EOM won’t scale across as high a proportion of a participant’s Medicare A/B population compared to OCM.
In addition, a more limited patient population included in EOM relative to OCM notably excludes a large population of patients that were a key driver behind the lack of aggregate savings in OCM at the model- level. OCM Participant’s found that cost performance in these episodes were particularly susceptible to extreme outlier effects because of their inherently low target expenditures and outcomes that were not reasonably within an oncologist’s influence in this population. For example, any patient receiving adjuvant hormonal therapy who underwent an orthopedic surgery during their OCM episode could’ve easily been tens of thousands of dollars over target for episodes with target prices of around $5,000; whereas a patient that was being treated with chemotherapy and underwent the same procedure would at least have a higher target, potentially in the range of $35,00-40,000.
MEOS Payments
In the OCM, the Monthly Enhanced Oncology Services (MEOS) payment amount was $160 per beneficiary per month (PBPM). The entire $160 was included as episode expenditures and therefore counted against each OCM Participant’s total cost of care target. In the EOM, the MEOS payment amount is $70 PBPM for non-dual eligible Medicare beneficiaries and similar to OCM, the entirety of this amount will be included in the EOM Participant’s total episode expenditures and counted against their total cost of care target expenditures. MEOS payments for dual eligibles will be $100 PBPM of which $70 will be included in a Participant’s total episode expenditures and counted against their total cost of care target expenditures.
Impact
EOM participating practices will likely receive less than half the MEOS revenue per performance period relative to practices in OCM because of the combination of lower MEOS payment amounts PBPM and lower overall numbers of patients that will be attributed to the model. Aside from the $30 increase in MEOS revenue for dual eligible EOM patients (relative to non-dual eligible EOM population) MEOS revenue will serve as an advance payment on practice redesign and will ultimately be at risk in the total cost of care performance reconciliation.
Risk Arrangements for Performance-Based Payment (PBP) and Performance-based Recoupment (PBR)
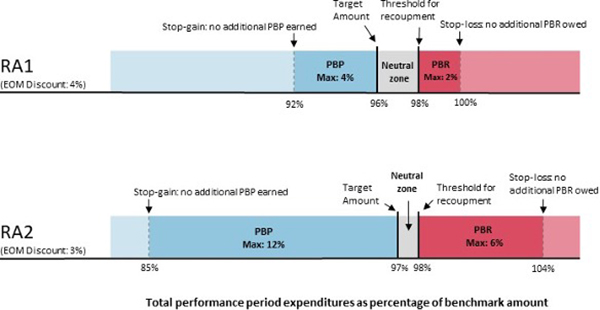
Whereas OCM risk arrangement options (RAs) included an upside-only option in which participants were not be penalized if aggregate episode expenditures exceeded Medicare’s target expenditures, EOM has two RA options that both include downside financial risk.
The less aggressive two-sided risk arrangement option (RA1) will include less total downside risk (below the generally applicable nominal amount standard for RA1 to qualify as an Advanced APM). However, RA1 will also include more limited upside compared to RA2, which is the more advanced risk arrangement option that offers greater upside in return for taking on higher financial risk.
Across both risk arrangements, if an EOM Participant’s performance period episode expenditures are in aggregate, higher than 98% of Medicare’s predicted total expenditures (i.e. “benchmark expenditures”), they would owe Medicare a performance-based recoupment (PBR). If an EOM Participant’s performance period episode expenditures are less than the target amount, then they are eligible to earn a PBP. Across both RAs, participants much achieve at least 2% savings relative to predicted episode expenditures to avoid a PBR. If participants’ actual episodes are in the “neutral zone,” meaning in between the target and the recoupment threshold expenditures, they would neither earn a PBP nor owe a PBR. In contrast, in OCM, practices did not incur any financial penalties if their actual episode costs were below Medicare’s benchmark total costs.
Impact
EOM participation involves substantially more financial risk relative to OCM because: (1) downside risk is mandatory for participation, with no upside-only option as was the case at the outset of OCM; and (2) the “neutral zone” is substantially narrower for EOM compared to OCM, and requires that practices generate at least 2% savings relative to predicted expenditures in RA1 and 1% savings relative to predicted expenditures in RA2.
Risk-adjustment for performance-based payments (PBP) and performance-based recoupments (PBR)
The episode pricing and risk adjustment model of OCM included a cancer care cost inflation factor (i.e. trend factor), novel therapies adjustment, and other episode price adjustment factors that were derived from each OCM Participant’s full population of episodes in aggregate.
In contrast, EOM will use cancer type-specific price prediction models, in which the trend factors, novel therapies adjustments, and application of other episode price adjustment factors will be disease-specific.
In addition, the final five performance periods of OCM included risk adjustments for breast, lung, and intestinal cancers based on metastatic (M1) status from participants’ clinical data reporting that participants were required to submit throughout the model. EOM will expand use of clinical data for target spending adjustments to include staging and HER2 status, and the RFA notes that further expanded use of clinical data for target spending adjustments may evolve throughout the model.
Impact
These methodology changes will likely help price targets keep pace with the use of higher-cost drugs as standards of care change throughout the model and decrease the extent to which practices are unfairly penalized (on the basis of cost) when utilizing costly immunotherapy regimens (such as checkpoint inhibitors or antibody-drug conjugates) in high-value indications.
However, even despite these methodology improvements in EOM, it’s not yet clear these changes will yield enough improvement to substantially limit the risk that EOM cost targets will align with changing standards of care for high-cost immunotherapy regimens in high-value indications, as described in the JAMA Oncology Viewpoint.
Required Practice Redesign Activities (PRAs)
The OCM participation required implementation of six Practice Redesign Activities (PRAs) aimed across key domains of oncology care delivery improvement. EOM will require two additional PRAs: (1) the gradual implementation of electronically submitted patient reported outcomes; and (2) screening EOM beneficiary health-related social needs (HRSN) using an approved screening tool and a specific health equity strategic planning requirement as part of the required use of data for continuous quality improvement (CQI).
Impact
The data collection and reporting burdens for the two new PRAs are likely to be significant. The six original OCM practice redesign activities were a heavy lift for practices already, and often required several years of iterative improvement initiatives to fully implement to point where patient care and outcomes were impacted. However, it’s important to keep in mind that improving health equity and specifically HRSN data collection is a top priority for CMS, and therefore CMS is considering expanding such data collection efforts outside of EOM (and even potentially including the Medicare Advantage population), which is a topic that we’ll discuss in more depth in our subsequent blog post on EOM and QPP participation options.
For any practice who seeks to apply to participate, CMMI will likely be favoring applications that include detailed and thoughtful proposals regarding how the practice proposes to utilize HRSN data (both from the participating PGP and aggregate HRSN data received from CMS) to improve health equity.
Data sharing and collection
In the OCM, participants were not required to collect any sociodemographic data, nor did CMS stratify data based on sociodemographic data within feedback reports or reconciliation reports. In the EOM, participants are required to submit sociodemographic data, if available, as a part of EOM health equity strategy. CMS may share with EOM participants certain aggregate, de-identified data, for example, aggregate utilization data, stratified by sociodemographic metrics (e.g., dual status, LIS eligibility, and race and ethnicity)
Impact
The additional data collection and reporting burden will likely be substantially higher than OCM (which was already very burdensome). Combined impact of lower MEOS revenue and mandatory two-sided risk is going to put a major strain on practice resources needed for data reporting.
CMMI has identified potential sources of selection bias among participants and their patient populations to watch. Health system affiliated cancer centers that have been collecting this data already because of participation in the Accountable Care Organization (ACO) Reach program might have a head start on this relative to community practices that haven’t been aligned to an ACO Reach participant. This could skew the patient populations in the model. Moreover, participants that have been active in research in health equity will likely have head start in preparing to collect these data. This could skew the patient populations in the model.
Differences between OCM and EOM are interconnected in their impact on financial risks that are inherent in participation
Below we’ve described a few examples of how key differences between OCM and EOM are interconnected and combine to have a significant impact on the financial risk associated with participation in the model.
Risk arrangement selection should consider the differences between the patient population included in EOM compared to OCM.
Like OCM, either EOM risk arrangement will qualify as an Alternative Payment Model (APM) within the Merit-based Incentive Payment System (MIPS) under Medicare’s Quality Payment Program (QPP). Any practice participant in either risk arrangement will qualify as a MIPS APM Participant. MIPS APM Participants face some reduced reporting burden in the MIPS program because the Practice Redesign Activities and Quality Measures that are included the EOM can substitute for some correlated MIPS reporting requirements.
Any practice participant in RA-2 will have the potential to qualify as an Advanced APM (Adv.-APM) participant in QPP, if the participant meets the thresholds that Medicare sets each year pertaining to the proportion of Medicare patients or total practice Medicare revenue managed within the Adv.-APM. Whether or not practice participant qualifies as an Advanced APM yields an additional increase in revenue opportunity and substantial reduction in MIPS reporting burden relative to MIPS APM participation.
However, since the included patient population in EOM will be significantly smaller than OCM, it is much less likely that a practice that participates in the more aggressive risk arrangement option (RA-2) will have the patient count or total dollars managed within the APM to qualify for Advance APM participation.
New documentation requirements have a significant impact on PBP methodology
In the final five performance periods of OCM, CMMI implemented a “metastatic” risk adjustment for OCM cost targets in breast, intestinal, and lung cancer. In doing so, Medicare raised or lowered a practice’s cost targets based on whether the clinical data that the practice reported for the episode included an M1 diagnosis (M1, M1a, M1b, M1c, pM1, pM1a, pM1b, pM1c).
The clinical data reporting requirements of EOM are likely to increase relative to OCM, and the EOM RFA clearly suggests that there will be “a more robust use of EOM participant- reported clinical and staging data in risk adjustment, to include ever-metastatic status and HER2 status.” The RFA also foreshadows that other target cost adjustments could be added throughout the model, noting that CMMI “would consider risk adjustment for social risk, if appropriate” based on data collected throughout the early years of the model.
Risk arrangements and PBP methodology impact the contribution of MEOS payments to practice transformation
In stark contrast to OCM, there is no “upside-only” risk arrangement available for practices to elect at the outset of EOM. This means that practice participants will be subject to varying degrees of downside financial risk in EOM if practices fail to manage the cost of EOM episodes below the cost targets that Medicare will set for included diagnoses.
Also, in stark contrast to OCM, PBPM MEOS payments that Practices will be eligible to receive in EOM will be far less than the $160 PBPM payment that they were eligible to receive in OCM.
In OCM, the entirety of these payments were included in the total cost of care for a practice participant’s patient population and measured against CMS calculated cost targets. In the EOM, MEOS payment amounts will be $70 PBPM for non-dual eligible (Medicare/Medicaid) patients; or $100 PBPM for dual eligibles of which $70 will be included as episode expenditures in reconciliation.
Therefore, in the upside-only risk arrangement in OCM, MEOS payments could be fully utilized to support a participant’s practice transformation initiatives, for example, the human resources and technology costs associate with required Practice Redesign Activities, notably including clinical data and quality measure reporting. However, in EOM (with the exception of the small portion of MEOS payments that are linked to dual eligible patients), since both of the risk arrangement options include downside risk, the MEOS payments should be thought of as an “advanced payment” to support Practice Redesign Activities, however these payments are essentially fully at risk of having to be paid back to Medicare based on a Participant’s cost performance in the model. This same concept applied to the two-sided risk option under OCM, however in OCM, the higher MEOS payments provided in the two-sided risk option still provided a materially better opportunity to underwrite investments in Practice Redesign through advanced payments (even though those payments were fully at risk).
Therefore, EOM is increasing the clinical data and reporting requirements relative to OCM but placing providers fully at risk for all costs associated with patient care, including payment that are collected throughout the model (with the small exception of $30 PBPM for dual eligibles). In a subsequent blog, we discuss in more detail some of the advantages and disadvantages the various options for participation in QPP and how those options related to the opportunity that oncology PGPs who submit an EOM application will have.